Reviewing Charles Richet’s work on anaphylaxis, awarded the Nobel Prize in 1913.
By Sasha Latypova
Source: sashalatypova.substack.com
Remember this quote? Credit
The 2nd shot, 21 days apart. Why the 2nd shot and why 21 days, exactly? Let’s take a look.
The anaphylaxis research history.
Charles Robert Richet (25 August 1850 – 4 December 1935) was a French physiologist at the Collège de France and immunology pioneer. In 1913, he won the Nobel Prize in Physiology or Medicine “in recognition of his work on anaphylaxis“. Richet devoted many years to the study of paranormal and spiritualist phenomena, coining the term “ectoplasm“. He believed in the inferiority of black people, was a proponent of eugenics, and presided over the French Eugenics Society towards the end of his life.
I would like to acknowledge that I knew not much about anaphylaxis other than it is a dangerous, life threatening allergic reaction. I witnessed it in a local grocery store pharmacy that administered covid vaccines. A young apparently healthy man (in his 30s) dropped on the floor immediately after the injection and was lying there when I walked in. Everyone was behaving like it wasn’t a big deal. I wanted to be let off this planet.
While working on this article, I ran a quick CDC VAERS query. All vaccines for all time in VAERS (about 30 years) produced 12,200+ anaphylactic reactions and 2200+ shocks. Covid-19 vaccines produced 9,000+ anaphylactic reactions and 1000+ anaphylactic shocks. mRNA injections are responsible for 11k of the total 12k reported anaphylactic reactions. However, that’s not the entire story of anaphylaxis.
Katherine Watt pointed me to Charles Richet’s Nobel Prize acceptance speech and to a couple of articles by this author (Northern Tracey). I suggest you read them. The author was way ahead of all of us on this topic.
Katherine published on our email exchange at the time:
Intentional elusivity of definitions for virus and vaccine.
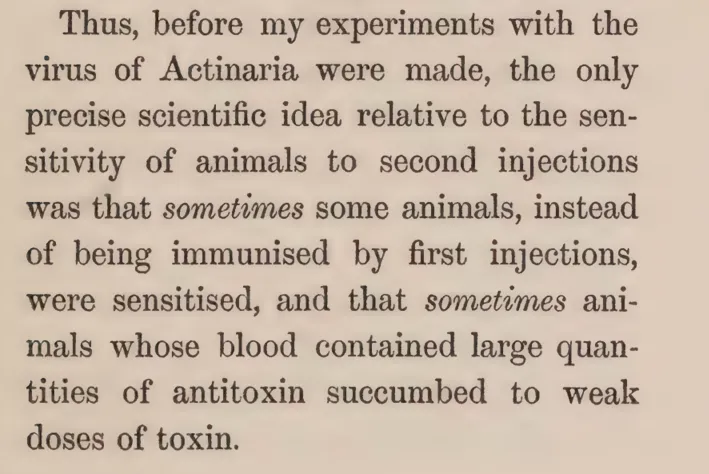
As I mentioned in my email exchange with Katherine, Richet’s own work clearly referred to the poison he made from tentacles of Actinaria (sea anemone) as the “virus of Actinaria”. This confirmed one more time what we already knew: viruses are not some sort of natural “seeds” of disease, randomly flying around and jumping strangers. They are poisons – either natural toxins excreted by plants, bacteria and animals, or poisons made by people like Richet and now CDC/pharma. They do not transmit by air or casual contact. (Editor’s note: This contradicts the article by Dr. Michael Palmer published by OVALmedia. We will continue to work on finding the truth. We consider both Sasha Latypova and Michael Palmer to be very competent).
What becomes apparent from reviewing Richet’s 100+ year old research – the only thing you really need to worry about with respect to “viruses/poisons” is an injection of biologics (proteins) for the 2nd time within the anaphylaxis window that starts typically after 20 days and lasting anywhere from months to years to the lifetime. This can happen in nature from the 2nd bite of an animal/insect carrying same biological toxin (a very low probability event nowadays), or from what is now forced by the government policy – from the needle wielded by a brainless money whore masquerading as a healthcare provider who is doing it for the 90th time in your or your child’s life “because science”.
The original biologics regulation law in 1902 was called the virus-toxin act. Early on, virus, toxin, antitoxin, serum and vaccine were used interchangeably, because the vaccinators knew what they were propagating in the labs and licensed establishments – biological poisons.
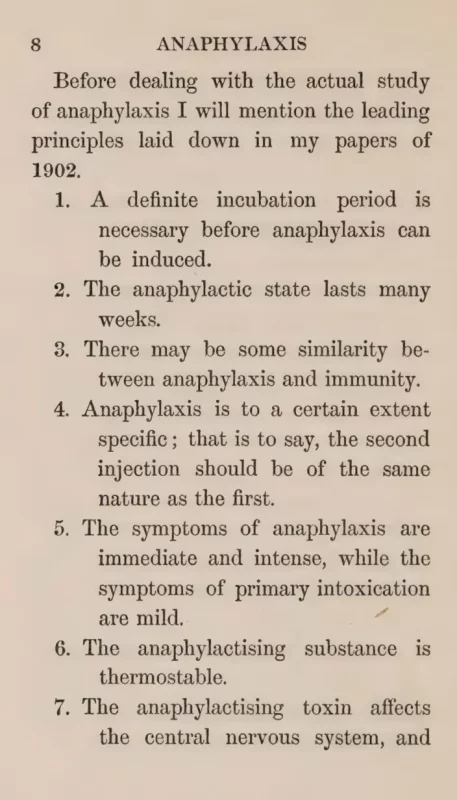
This lead me to become intensely interested in Richet’s work. I found his book describing the work on anaphylaxis published in 1913. I am including several screenshots from it, so you can read for yourself.
Richet alluded to vaccination being a failure from the first attempts, because, instead of producing expected immunity it produced violent reactions or even death from minute (not considered dangerous) amounts of the toxin at the 2nd exposure. This happened in a random % of the population. One example quoted anaphylaxis rates from injecting cattle with anthrax serum: approximately 10% became violently ill and many died. The population who would react anaphylactically is a-priory not distinguishable from others, because it is not known who is already sensitized to which biological substances.
This is still the case. There is no way to determine upfront who will be anaphylactically sensitized by an injection of a biologic (a protein). The establishment healthcare denies this, proclaiming all vaccines “very safe”. This is categorically not true, as becomes very apparent once you read Richet’s work related to injecting biological substances, even benign ones like milk or albumins (derived from wheat and other cereals). Digesting a protein and injecting it directly into the blood stream are two entirely different things! For example, it is safe to ingest snake venom for most people (provided no sores or abrasions in the mouth). I am not advising you try this, but sucking the venom out immediately post bite has been used as a bush medicine method. However, a snake bite delivering the same venom directly into the blood stream is an entirely different story.
You notice that Richet talks about the “second injection”. This refers to the nature of anaphylaxis: the first interaction with an injected toxin may be not even noticed, be well tolerated or may be at worst mildly irritating. After a period of 2-3 weeks, the second exposure, however, may become very dangerous or fatal. The second exposure in most of Richet’s experiments was by injection. However, with high enough sensitization by the first injection, the anaphylaxis could also result from environmental exposure or ingestion, depending on the degree of sensitization to the “allergen”, or “toxigen” as he termed it. Do you understand peanut allergy, gluten allergy, soy allergy, etc. now? The things that didn’t exist before peanut oil, wheat albumins and other common food proteins became widely used in vaccines (and were proclaimed “generally safe” because it’s just food).
Importantly, Richet has demonstrated that anaphylaxis, anaphylactic shock and the variety of allergic reactions are all the same phenomenon, stemming from the same thing – a sensitizing exposure by proteins reaching the blood stream and bypassing normal digestion.
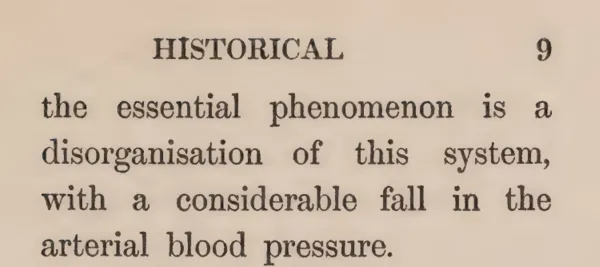
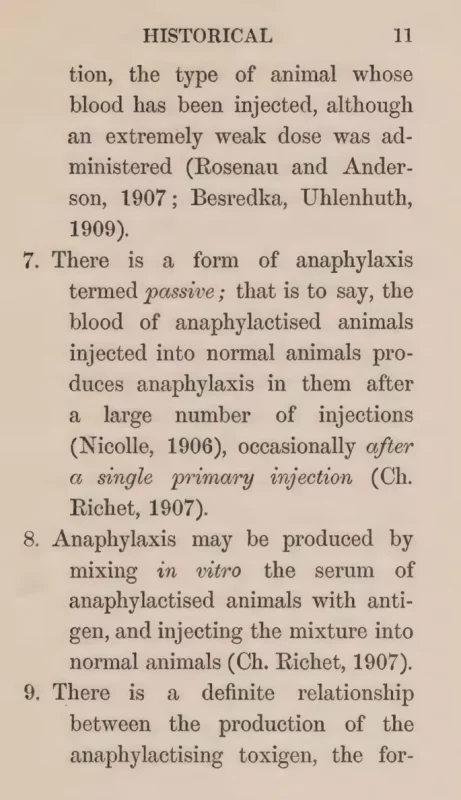
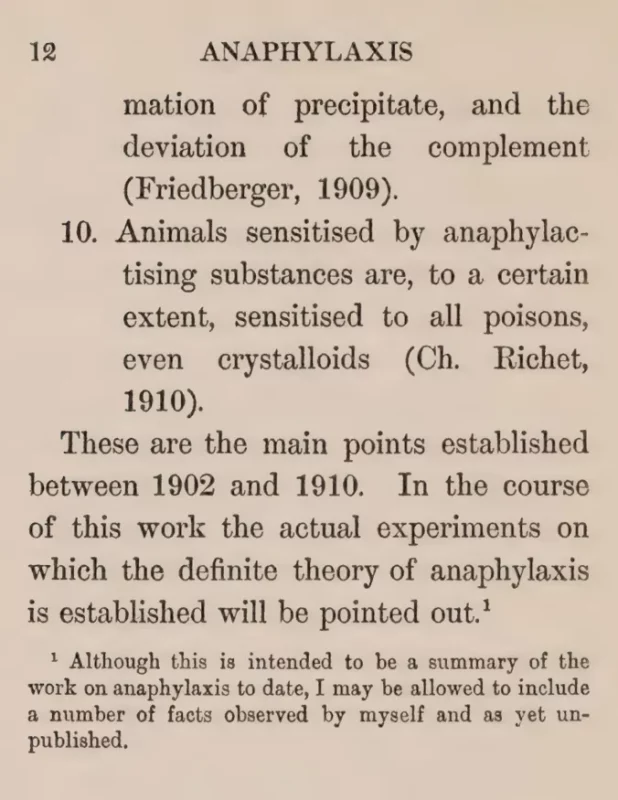
Richet provided principles of anaphylaxis in his book:
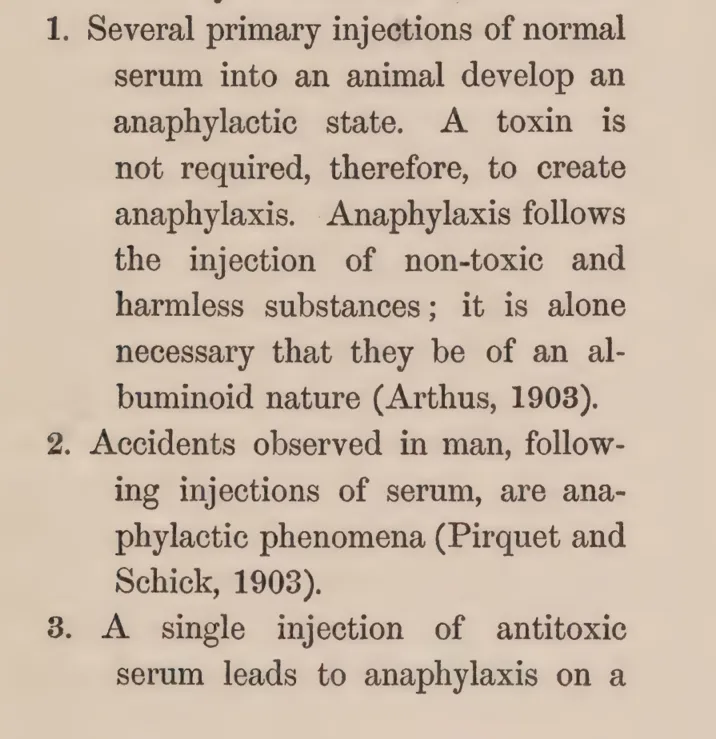
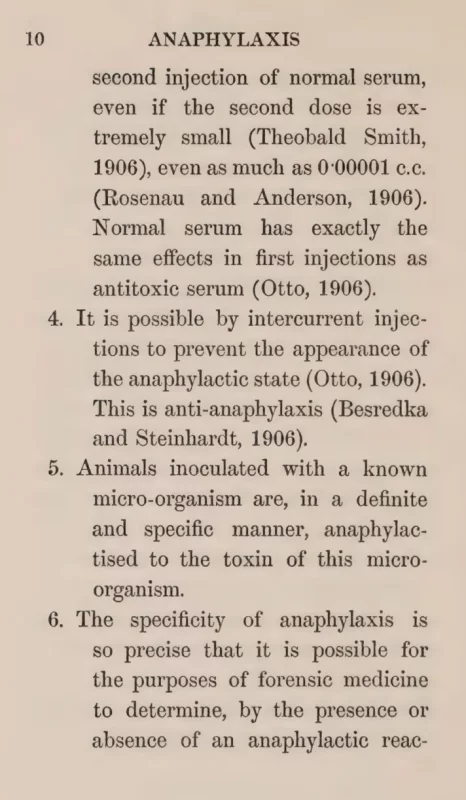
He also summarized findings from other researchers working on anaphylaxis at the time. Notice especially points 8 and 10 – this describes anaphylaxis from “vaccination” and subsequent allergic reactions, even to non-proteins (crystalloids):
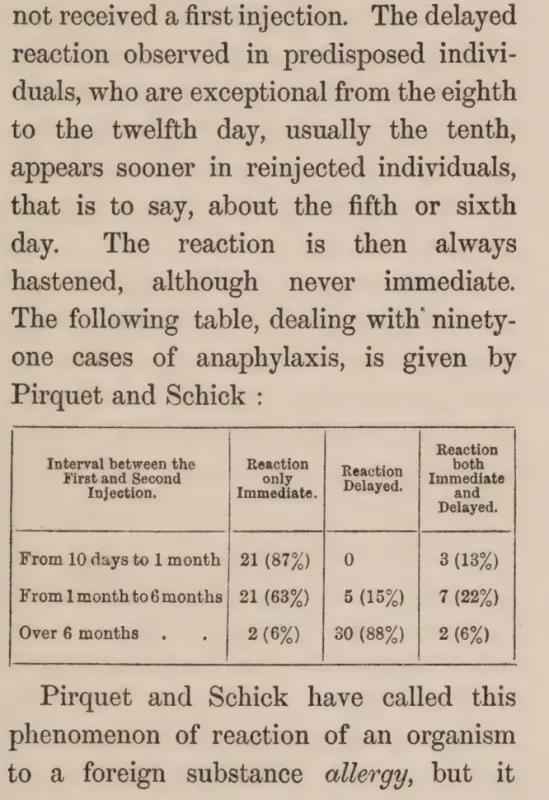
Richet found that the state of anaphylaxis sets in after a period of 2-3 weeks (it can vary), and depending on the initial toxin/protein, the sensitization state may last from weeks to years, and possibly be permanent. At the time that he wrote the book, he mentioned that in people anaphylactic/allergenic state was observed up to 6 years, but it may be permanent. Do you see now, why most vaccines are delivered in at least 2 doses, and they are separated by at least 21 days? They want to see if they induce severe anaphylaxis (i.e. life threatening kind). Here’s Pfizer’s “postmarketing experience” document, compiling adverse events as of Feb 2021 (first 2 months of vaccine rollout):
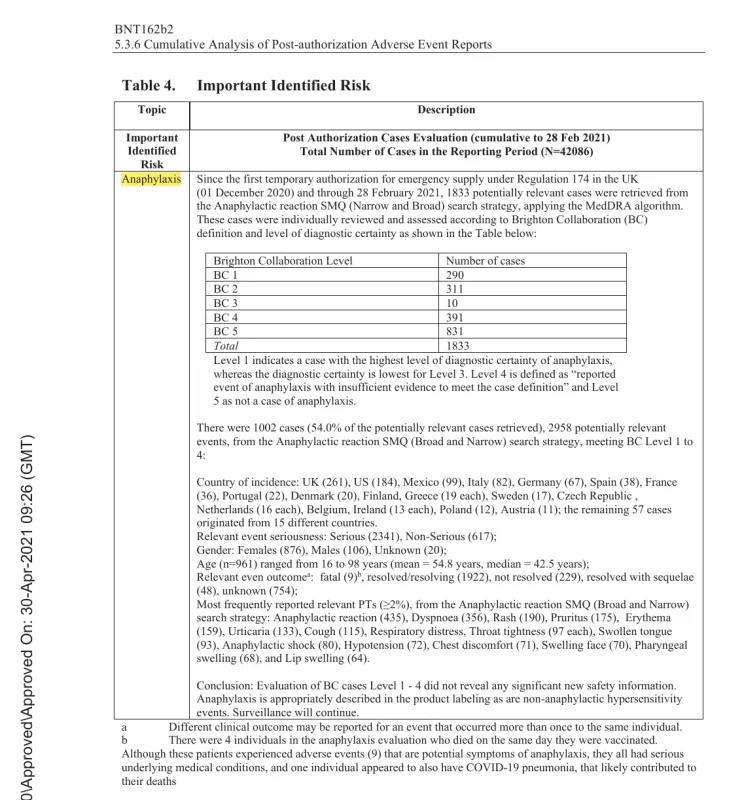
This table is is not all cases of anaphylaxis, of course, but only the most severe form – the shock.
Anaphylaxis is all allergic reactions and autoimmune disease, but these things are very easy to deny as they take a while to manifest and are not immediately deadly. The industry has developed perfect gaslighting strategies: “genetic mutations”, “toxic food”, “stress”, “novel syndromes”, and even better – glorification of chronic illness via movies, advertising, non-profits and other economic activity feeding off vaccine-induced destruction of natural health. In case of mRNA vaccines, they absolutely knew that they are killing people with anaphylaxis, but since that was the goal of the military weapon, the shots have not been removed and continue being pushed on the public.
Another interesting observation made by Richet is that white mice and some of the breeds of rats do not experience anaphylaxis. No wonder these animals are now the staple of pharmaceutical research!
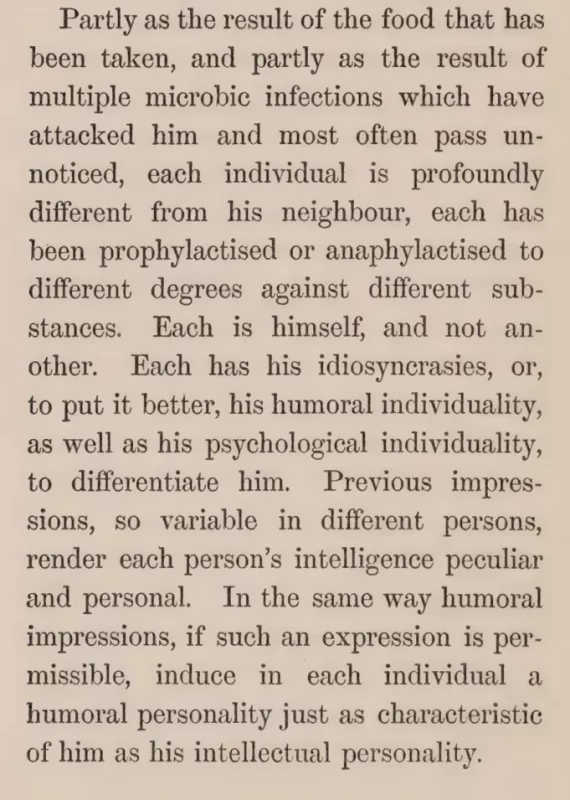
While Richet himself seemed to be very much pro-vaccination, his main conclusions about anaphylaxis speak soundly against it. It is impossible to design a safe vaccine, because it is impossible to predict anaphylactic reactions. Each individual is unique, a product of heredity and interactions with environment. Introduction of foreign, non-self proteins is an assault on this natural equilibrium and can only result in a disaster.
That vaccination in people induces anaphylaxis was known early on:
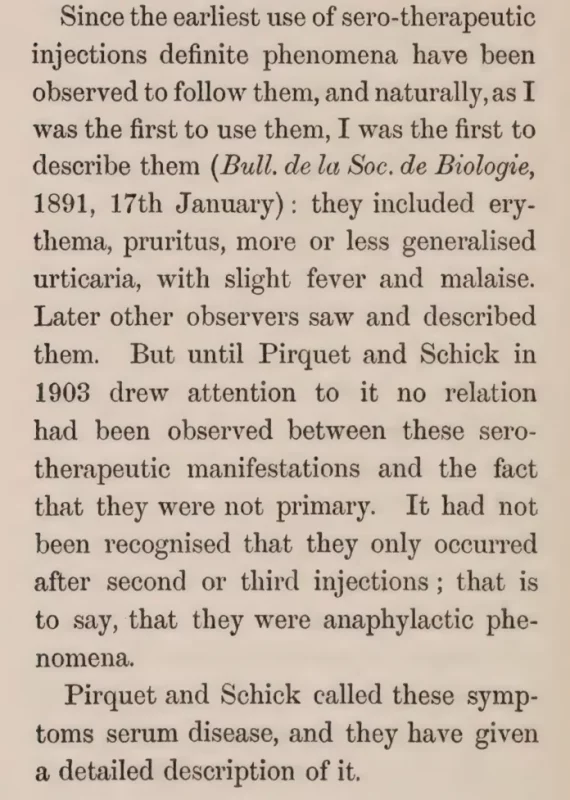
And was given the name “allergy”, possibly to hide the fact that it’s vaccine-induced anaphylaxis:

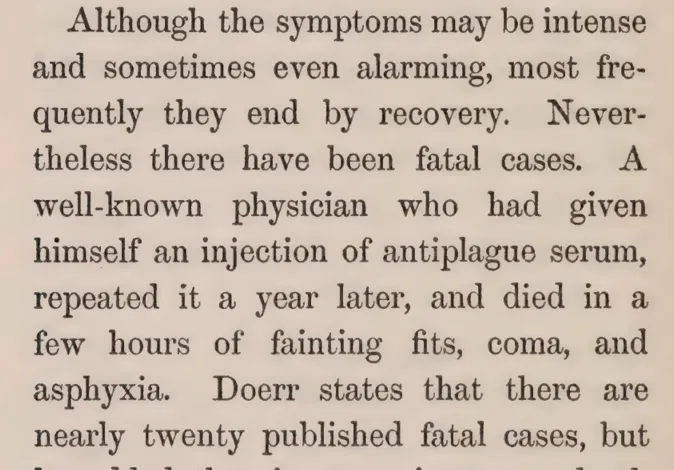
These psychos would even kill themselves, and still not get the message:
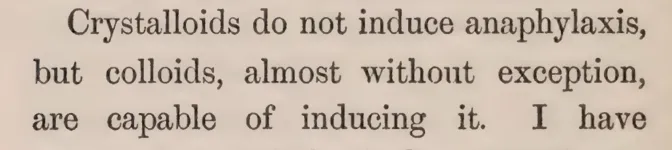
Substances that induce anaphylaxis – colloids.
Colloids vs crystalloids
Colloids and crystalloids are two types of fluid solutions used for intravenous (IV) infusion in medicine. The primary distinction between them lies in their particle size, composition, and behavior in the body.
Colloids
- Consist of large particles (0.5-100 nm) that do not pass through semi-permeable membranes, such as capillary walls
- Examples: gelatin, albumin, hetastarch, dextran
- Act as plasma volume expanders, maintaining blood volume and pressure
- Have a high oncotic pressure, which helps to draw fluid into the vascular compartment
- May cause anaphylaxis in some patients
- More expensive than crystalloids
- Suitable for patients with severe fluid loss, trauma, burns, or sepsis
Crystalloids
- Consist of small particles (less than 0.5 nm) that can pass through semi-permeable membranes
- Examples: normal saline (0.9% NaCl), lactated Ringer’s solution, 5% dextrose in water
- Act as isotonic or hypertonic solutions, expanding extracellular fluid volume
- Have a lower oncotic pressure, which can lead to fluid accumulation in tissues
- Less likely to cause anaphylaxis
- Generally less expensive than colloids
- Suitable for patients with mild to moderate fluid loss, dehydration, or electrolyte imbalance
In general, small molecule drugs do not cause anaphylaxis.
Vaccines are, of course, colloids as they contain a mixture of proteins and lipids in suspension.
Properly matched blood transfusions do not generally produce anaphylaxis. However, since all blood banks are now contaminated with mRNA-injected blood, it is not possible to say that they are safe. I personally would not accept blood, except from a known donor.
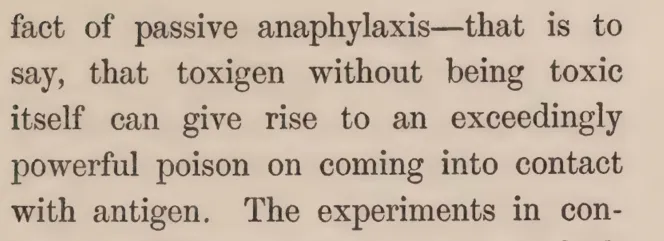
Richet proposed that a “toxigen” which developed after the initial sensitizing injection in the blood was responsible for subsequent state of anaphylaxis:
“Infectious disease” explained by anaphylaxis:
The phenomenon of anaphylaxis may help explain both, the natural outbreaks of what appears as “contagious illness” in human history and the skyrocketing chronic illness in the modern western populations. It is known that the bacteria implicated in diseases like cholera or the plague are commonly present in the intestinal tracts of many people and do not seem to cause any issues. Then, how does an epidemic of the plague or cholera occur? Imagine living in a crowded, rapidly growing European city around 15th – 17th century:

This is one of the main streets in Amsterdam, with raw sewage flowing in the middle, domestic animals sharing lower floors of the buildings, no plumbing, sanitation or refrigeration of food. The rats are very common. They bite and the bites carry common proteins found in that area’s sewage. Once enough people in the same area have been bitten for the first time, some weeks go by, anaphylactic state develops, and then the rats bite some of the same people again. If enough of these events occur, an “epidemic” of the plague/smallpox/cholera starts in this community.
Hygiene, plumbing, water sanitation, refrigeration and air conditioning were the most significant technological innovations that defeated epidemics by removing the chances of injection of anaphylactizing toxigens by common pests. So, instead, we now have the establishment “healthcare” assaulting the society like the medieval sewer rats with poisoned needles. All vaccines contain two main sources of injury – the proteins that are used to formulate them, including the toxins (“viruses”) and the vehicle which frequently contains other common proteins like albumins (gluten allergy), egg proteins, soy, corn, casein (milk intolerance), etc. There are also “contaminants” and “adjuvants” such as toxic metals, and more recently with introduction recombinant vaccines – DNA plasmids that transfect cells. The mRNA shots are even worse as they contain numerous toxic vectors. Now imagine a baby getting 70+ different shots, most in several doses. It is guaranteed that the baby will get anaphylactized to many commonly encountered proteins, and that a chronic inflammation/allergy will result. Anaphylaxis, being an intestinal reaction, is also tied to destruction of microbiome, which I will address in later articles. Practically all chronic conditions, especially in children, can be tied back to vaccine-induced anaphylaxis.
Many people state that food that we eat and the environment are full of toxins. While this may be true, especially for some locations and some socioeconomic groups, the food and environmental toxicity pales in comparison to what happens when the toxins, especially proteins are injected directly into the blood stream. I am in full support of improving the quality of food and cleaning up the environmental pollution, but if we need a policy to combat the chronic disease epidemic, there is one straightforward answer that all politicians and most experts today soundly ignore – the catastrophic damage to health induced by vaccines.
I would like to end with the quote from Richet:
Richet: “We are so constituted that we can never receive other proteins into the blood than those that have been modified by digestive juices. Every time alien protein penetrates by effraction [forcible entry; injection], the organism suffers and becomes resistant.
This resistance lies in increased sensitivity, a sort of revolt against the second parenteral injection [outside the intestines; intravenous, intramuscular, or subcutaneous] which would be fatal.
At the first injection, the organism was taken by surprise and did not resist. At the second injection, the organism mans its defences and answers by the anaphylactic shock. Seen in these terms, anaphylaxis is an universal defence mechanism against the penetration of heterogenous substances in the blood, whence they can not be eliminated.”
For further reading:
How Much Damage Have Vaccines Done to Society?
Art for today: Angels and Demons series, oil on linen. NFS.